Diabetes Awareness
My first husband, Howard, died of pancreatic cancer at the age of 58. We had been together off and on since the age of 20, so of course this was a terrible loss for me. Unfortunately, we had no idea of the early warning signs of pancreatic cancer and its relationship to diabetes. Howard had been diagnosed with Type 2 diabetes a few years before his cancer diagnosis. He was taking Metformin and seemed to be doing okay. However, he was a long-distance truck driver and found it hard to eat a low-carb diet while on the road.
This was how things began. One day Howard was on his way home with his 18-wheeler, which was empty, as he had finished his deliveries. He was about an hour from Pittsburgh on a winding, narrow, mountainous road when he completely lost his eyesight. This sounded so odd to me, as I knew him to have 20/20 vision. Howard made a call to his boss who arranged for another two drivers to meet him. One to take him to the emergency room and the other to bring the truck back to the yard.
The doctor who examined Howard said his blindness was due to sudden onset diabetes and he would recover within 30 days and at that time would be able to return to work. Surprisingly, that is exactly what happened. His eyesight returned to a vision of 20/30 in about a month, and he was able to return to work. This just seemed so odd to me. Howard was referred to an endocrinologist and was put on a regimen of Metformin and advised to change his diet and get a bit of exercise. This seemed to work well for a few years until Howard needed a knee replacement. He was 6’4″ and in his younger years he used to play a fair amount of basketball, which resulted in a lot of injury to his knees. he also worked for a time as a long-distance mover, which certainly didn’t help, and his current job involved heavy lifting. His right knee was giving him a lot of trouble and his primary doctor said it was time to get it taken care of. A surgery was planned and the operation was performed successfully. All was good. He began his physical therapy.
About a week after the operation, Howard began to complain about stomach pain and nausea, itching, light colored stools, and said his eyes were yellow. I couldn’t see this, however. He called his physician who had performed his operation and was told to meet him at the hospital. I was scheduled to do a television interview the next morning to promote my newly published cookbook, The Diabetic Pastry Chef and had a lot of prep to do, but felt it was important to support my husband with his illness, so I went to the hospital with him.
We were at the hospital for a lengthy amount of time and all manner of tests were done, including a Cat Scan. Imagine our shock and dismay when the doctor came into the room and broke the news to us that the tests came back with some troubling news. The doctor held up an image from the Cat Scan machine showing Howard had pancreatic cancer! This was unbelievable! I mean how do you go from a knee replacement to being told you have pancreatic cancer! I’ll be honest, the first thing I thought about when we got the diagnosis was how the old folks back in the day would say, never let them open you up for an operation. because if you have cancer it is going to spread! Not sure how true this is, but we had no idea Howard even had cancer! Crazy thoughts enter your head when you’re suddenly given such frightful news. The whole thing became a blurry whirlwind of doctor’s appointments, hospital visits, chemo and radiation treatments, and I was expected to promote my cookbook at the same time! The doctor explained if everything did not turn out well, the most dire prognosis would be Howard had 6 months to live. Howard died right about the 6 month mark.
I tell this story in the hopes it might help someone with sudden, new onset diabetes to be alert that this could possibly be the first sign that pancreatic cancer might be developing. We had no idea at the time that there could be a connection between sudden onset diabetes and pancreatic cancer. Not many people are aware of this. Also, I’d be remiss if I didn’t add, Howard was a pack a day cigarette smoker. I’m sure this also contributed greatly to his outcome.
My late husband, Howard
Could a Diabetes Diagnosis Help Detect Pancreatic Cancer Early?
July 7, 2021, by Sharon Reynolds
Bob Aronson was only 54 years old and, in the words of his son Tom, “extremely healthy.”
“So it was really surprising to everyone when he went in for an annual routine eye exam and his eye doctor suspected diabetes,” Tom recalled.
With his diabetes diagnosis confirmed, Bob got back to his normal routine, with the addition of daily blood sugar checks. But only a year after that trip to the eye doctor, he received a diagnosis of metastatic pancreatic cancer. He died 9 months later.
Around the time of Bob’s cancer diagnosis, in 2005, Tom overheard some of his doctors mention a growing suspicion of a possible link between a new diagnosis of diabetes, sometimes called new-onset diabetes, and pancreatic cancer. In other words, in rare cases, diabetes may actually be caused by a tumor in the pancreas.
Though the Aronson family can’t know if Bob’s diabetes was caused by his tumor, “we’ll always wonder what would have happened if he could have been tested [for pancreatic cancer] the second he presented with diabetes?” Tom asked.
Over the last several years, evidence has mounted to support a link between new-onset diabetes and pancreatic cancer. And the Aronson family’s hope has been inching closer to reality: Several large NCI-supported studies are testing ways to pick out those people whose diabetes might be a sign of a much deadlier problem. The research is part of larger ongoing efforts aimed at finding ways to detect pancreatic cancer early, when treatments may be more effective.
“There’s been a lot of progress over the last 5 years or so,” said Brian Wolpin, M.D., M.P.H., who leads a pancreatic cancer early detection program at the Dana-Farber Cancer Institute. “We’re not quite to the point where there’s a test in the clinic that you can order, but we’re getting progressively closer.”
Risk as a Two-Way Street
Although pancreatic cancer is only the 11th most common cancer in the United States, it’s the 3rd leading cause of death from cancer. Unlike breast, colorectal, and lung cancer, no screening test exists to catch it early.
More than 80% of the time, people are not diagnosed with pancreatic cancer until after it’s invaded nearby tissues or spread to other organs. And, overall, only about 10% of people with pancreatic cancer will be alive 5 years after their diagnosis. But about 40% of people diagnosed before their cancer has spread outside the pancreas will be alive after 5 years, highlighting the importance of early detection.
An important job of the pancreas is to produce insulin. This hormone controls the amount of sugar in the blood by moving it into cells, where it can be used by the body for energy. In type 1 diabetes, which is relatively uncommon, the immune system attacks and destroys the cells in the pancreas that make insulin.
Type 2 diabetes, which affects almost 10% of the US population, is usually the result of the body not being able to properly use the insulin it makes. Being age 45 or older, having a family history of diabetes, or being overweight are risk factors for developing type 2 diabetes.
Physical inactivity, race, and certain health problems such as high blood pressure also affect the likelihood of developing type 2 diabetes.
And living with diabetes for a long time “is a known risk factor for pancreatic cancer,” said V. Wendy Setiawan, Ph.D., of the University of Southern California, who’s led long-term studies of pancreatic cancer risk in diverse populations. The reasons why aren’t totally clear, but some of the proposed mechanisms include higher-than-normal levels of insulin circulating in the blood, high blood sugar, and long-term inflammation caused by type 2 diabetes, she explained.
But in some people, diabetes can rapidly develop because of a problem in the pancreas, instead of the diabetes causing damage to the pancreas in the long run. These problems can include chronic inflammation of the pancreas, cystic fibrosis, and pancreatic cancer.
“Anything that damages your pancreas can [cause it to] not make enough insulin,” said Dr. Setiawan. The result of this damage can be a rare kind of diabetes sometimes called pancreatogenic diabetes or type 3c diabetes.
This type of diabetes is very uncommon, explained Anirban Maitra, M.B.B.S., of the University of Texas MD Anderson Cancer Center. “In the overwhelming majority—more than 99%—of new cases of diabetes, it’s just run-of-the-mill type 2 diabetes,” Dr. Maitra explained. But the other 1% with pancreatogenic diabetes have a risk that their diabetes is driven by pancreatic cancer.
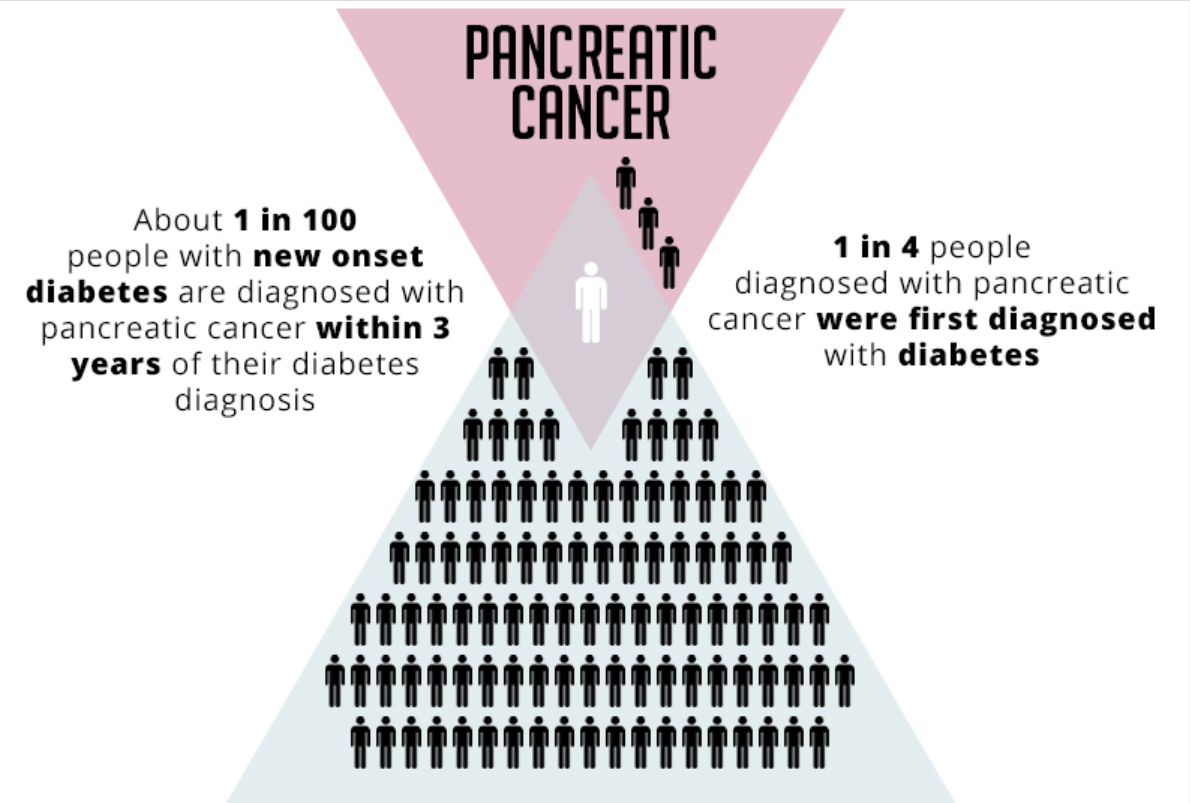
While frightening, this last scenario is rare—the estimates are that fewer than 1 in 100 cases of new-onset diabetes are caused by cancer. And about 1 in 4 people diagnosed with pancreatic cancer were first diagnosed with diabetes.
“So how do we pick out that small, small subset of people with pancreatogenic diabetes, which in some cases may be caused by cancer?” asked Dr. Maitra.
Finding Those at Highest Risk
At the moment, there’s no good answer to that question. Sending every person with new-onset diabetes to get imaging tests of the pancreas would result in too many unnecessary follow-up surgical procedures—when abnormalities seen on scans turn out not to be cancer—potentially doing more harm than good, explained Suresh Chari, M.D., also of MD Anderson.
To help find these rare patients with pancreatogenic diabetes while limiting harms, including unnecessary surgeries and the fear caused by undergoing diagnostic procedures, Drs. Chari and Maitra are leading a nationwide project, funded by NCI and the National Institute of Diabetes and Digestive and Kidney Diseases, called the New Onset Diabetes (NOD) Study.
The project, which is in the process of enrolling 10,000 people with new-onset diabetes or hyperglycemia (also known as prediabetes), hopes to develop a blood test that can identify the few individuals who may need further testing for pancreatic cancer, Dr. Maitra explained.
“Can we identify biomarkers in the blood that will tell us, in a room of 100 patients with new-onset diabetes, there may be someone who we need to send for more workup and imaging studies?” he asked.
Out of 10,000 participants, Drs. Chari and Maitra estimate that about 85 will develop pancreatic cancer during the study.
Participants will donate blood samples periodically for up to 3 years. The NOD researchers will look for proteins and other biomarkers found in samples that differ substantially between people who later develop pancreatic cancer and those who don’t. Their hope is to find a specific group of markers in the blood that can be used in the future to detect those people with new-onset diabetes who are at highest risk for pancreatic cancer.
Such markers could then potentially be used as the basis of a test that, “when a patient walks in with new-onset diabetes, can raise a red flag that they should go and get some additional tests” for pancreatic cancer, said Dr. Maitra. And ideally, such a test would help identify the cancer long before it has spread beyond the pancreas.
“The longer you have to wait, the closer you’re getting to the clinical diagnosis of pancreatic cancer and losing that window of opportunity” for early detection, Dr. Maitra said.
A Trial for People at Highest Risk
Since Bob Aronson’s diagnosis more than 15 years ago, researchers have come to recognize that several clinical factors can also be used to identify a subset of people with new-onset diabetes who have an especially high risk of pancreatic cancer.
Three key differences that tend to be found together distinguish these people from others with new-onset diabetes, said Dr. Maitra. “One is their age,” he explained. People who develop diabetes as a consequence of pancreatic cancer tend to be older, he explained.
The second is that blood sugar levels tend to rise more rapidly in people whose diabetes is driven by a tumor. “And the third is weight loss,” Dr. Maitra explained. “Normally with type 2 diabetes, people gain weight when they become diabetic.” People whose diabetes is caused by pancreatic cancer can instead experience unexpected weight loss around the time of a diabetes diagnosis.
In 2018, Dr. Chari and his colleagues proposed that these three clinical risk factors, which they called the Enriching New-Onset Diabetes for Pancreatic Cancer (ENDPAC) score, may be useful for identifying people who need additional testing now, before a blood test has been developed.
Not long after, they found some groups willing to take them up on testing that idea.
If people with new-onset diabetes who have a high ENDPAC score are indeed more likely to have pancreatic cancer, said Lynn Matrisian, Ph.D., chief science officer at the Pancreatic Cancer Action Network (PanCAN), “as an advocacy group, our interest is: Can we help these people now?”
PanCAN recently launched the Early Detection Initiative (EDI) for Pancreatic Cancer, a collaboration with NCI and the Fred Hutchinson Cancer Research Center in Seattle. The initiative is testing whether referring people to get a CT scan of the abdomen based on a high ENDPAC score alone can find early-stage pancreatic cancer while minimizing unnecessary follow-up procedures, anxiety, and overdiagnosis. (Overdiagnosis is when a cancer that will never cause any symptoms is found, potentially leading unnecessary diagnostic procedures and treatments.)
As part of the EDI, CT scans will be stored in a repository. This resource could potentially be used for future studies using artificial intelligence-based approaches to improving pancreatic cancer imaging, explained Eva Shrader, PanCAN’s director of scientific initiatives.
The EDI is also contributing samples of blood from participants to the NOD study, “But we mainly want to answer the clinical question: Will imaging work for early detection for people with a high ENDPAC score?” said Dr. Matrisian.
Beyond Diabetes
In addition to diabetes, there are other established risk factors for pancreatic cancer, including a family history of pancreatic cancer or having a pancreatic cyst, explained Dr. Wolpin. However, most of the approximately 60,000 people in the United States who develop pancreatic cancer every year don’t have known risk factors for the disease.
“[Studies] suggest that survival for pancreatic cancer could be improved many-fold if we could detect it at early stages,” said Sudhir Srivastava, Ph.D., of NCI’s Division of Cancer Prevention (DCP). Since 2016, DCP’s Pancreatic Cancer Detection Consortium (PCDC) has been funding research teams to develop something that has proven elusive: a test that can detect pancreatic cancer early in people not already known to be at high risk.
Creating a blood test that could pick up early pancreatic cancer in the general population faces many hurdles, Dr. Wolpin explained. One is that, since about 80% of people with pancreatic cancer are diagnosed at a late stage, blood samples taken from people with pancreatic cancer largely reflect the biology of advanced disease.
Blood samples from people with early-stage pancreatic cancer are rare, Dr. Wolpin added. So he and his team are collaborating with cancer centers across the country to collect blood from people newly diagnosed with early-stage pancreatic cancer.
“This way we’ll be better able to capture a larger number of those patients,” he said. “Part of the benefit of the structure of the PCDC is that it helps us all collaborate to do that.”
They’re also following a large group of people at high risk of pancreatic cancer—those with a family history or with pancreatic cysts—over time. That includes periodically collecting blood and tissue samples.
“Unfortunately, some of these people will be diagnosed with pancreatic cancer,” said Dr. Wolpin. “When this occurs, we will have samples in the bank that are actually from before their diagnosis, before they got symptoms,” he continued.
Such samples may allow them to identify markers that can form the basis of a pancreatic cancer screening test for the general population.
There’s already some evidence to support that possibility. Recent work on a related project found that changes in levels of a protein called CA19-9, which is commonly used to track responses to pancreatic cancer treatment, can be found before diagnosis in blood samples from people who later developed pancreatic cancer.
However, on its own, CA19-9 was not sensitive enough to identify everyone who went on to develop pancreatic cancer. His team is now looking for other markers in the blood that show similar changes before a pancreatic cancer diagnosis.
Eventually, he explained, any blood-based markers to detect pancreatic cancer may be incorporated into what are called pan-cancer screening tests: those that screen for many cancer types at the same time.
Other PCDC teams are looking at different sets of proteins and other markers in the blood that may help with early detection, and ways to improve imaging of the pancreas. If doctors end up searching for smaller and smaller tumors, they get harder and harder to see on conventional CT scans, Dr. Chari explained.
Researchers are studying alternative methods that may be able to pick up tiny deposits of tumor cells, including ultrasound techniques that can visualize tumors as small as a millimeter, and PET imaging that homes in on proteins expressed specifically by pancreatic cancer cells. All these projects involve multidisciplinary teams that are committed to working together across institutions.
Early detection of pancreatic cancer “is very much an area where collaboration is necessary,” said Dr. Wolpin. “People sometimes believe that scientists work alone in their own labs and don’t talk to each other. That really is not true, particularly in this area. The PCDC, the NOD cohort, and the Early Detection Research Network are great examples of large consortia really working together to try to solve this difficult problem.”
“Pancreatic cancer is so deadly because there’s no early detection,” Tom Aronson said. “That’s why I’m so excited about all the work that’s happening now. Hopefully, in the future, many people who get pancreatic cancer won’t [be diagnosed] at stage 4, and there will be some hope for them and their families.”
If you would like to reproduce some or all of this content, see Reuse of NCI Information for guidance about copyright and permissions. In the case of permitted digital reproduction, please credit the National Cancer Institute as the source and link to the original NCI product using the original product’s title; e.g., “Could a Diabetes Diagnosis Help Detect Pancreatic Cancer Early? was originally published by the National Cancer Institute.”
